
Managing a portfolio/logbook of your training scans
As a former family physician/part time regional centre emergency room doctor, and as a physician who is currently refocusing on internal medicine and critical care (yes, I am back in residency), I am justifiably a point-of-care ultrasound (POCUS) enthusiast.
You are probably aware that various POCUS credentialing processes, specifically for those clinicians who did not receive longitudinal POCUS training during medical school or residency, often look somewhat like this:
Back in 2008, the University of Saskatchewan’s Department of Emergency Medicine embarked on a process much like the above by adopting the Canadian Point of Care Ultrasound Society’s (CPOCUS) certification program. It is currently the department’s primary POCUS credential, and it has served them well in terms of assuring basic competence amongst already-in-practice clinicians (over 80% of Emergency Physicians in Saskatoon have obtained basic CPOCUS certification). But as the number of acute care POCUS applications continues to grow – with now well established resuscitative, diagnostic and musculoskeletal applications – so too has the demand for robust training processes and improved training workflow. Incidentally, this same department just launched its own internal wireless image capture system (QPath) thus enabling a pretty slick training regime, but this post is for those eager POCUS learners whose departments aren’t quite there (yet).
One important evolution in these newer training schemes is the increasing role of image capture (specifically capture of real patient clips). CPOCUS, for example, now accepts up to 50% of training scans (of advanced applications) in the form of saved clips for review by their instructors.
To comply with the option of obtaining additional scans for review by your supervisor/ instructor, I do the following: I record de-identified clips, approximately 4 seconds long and insert them into presentation software. Choosing a convenient “split screen” slide, allows a video clip on the one side and an interpretation on the other. This is preceded by a short clinical vignette and rounded off with a short diagnostic summary.
I find that this keeps my clips and case information together and produces a visually pleasing, easy to follow log of my un-proctored scans. Reviewers can use the notes area for critiquing, questions or suggestions. Here is what a typical case ends up looking like:
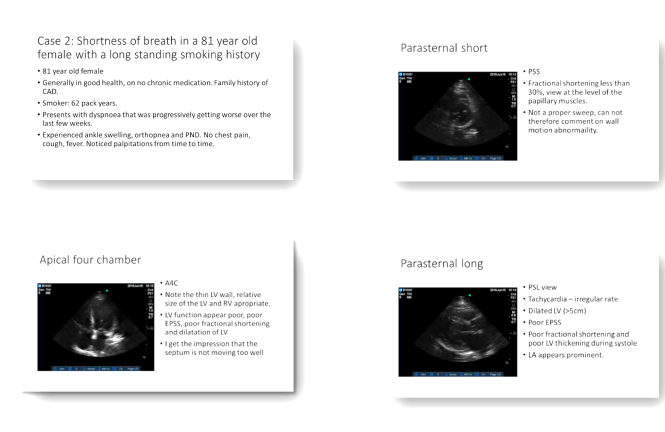
The few slides above illustrate a picture of an elderly lady with a longstanding smoking history presenting with shortness of breath. Her cardiac views would suggest a cardiac etiology as opposed to COPD for her symptoms. Scanning her lungs showed B lines in all fields. Her formal echocardiography was consistent with my bedside assessment and reported an EF of 30%. As a result of POCUS, heart failure treatment was initiated earlier.
This is how I keep my scans together. Feel free to use it! I would love to hear from others so please comment and tell us how you keep your scans together.
Dr Leon Byker, BSc MBChB CCFP; PGY2 Internal Medicine, University of Saskatchewan.
Peer Review by Dr. Paul Olszynski, Emergency Medicine, Director of Sasksonic, University of Saskatchewan
