
Our annual conference is coming together and we’re now accepting abstracts for our lightning oral abstract presentations. Each abstract submitted will be reviewed and scored by our team of reviewers. The top 5 abstracts will be awarded 8 minutes for presentation just prior to the SONOGAMES. Submission deadline is Feb 5th – details below!
Author: sasksonic
Case of the Year – Just in time for the Holidays!

As we wrap up another great year at Sasksonic, we are thrilled to learn that one of our own recently took home POCUS-Toronto’s “Case of the Year” award!
USask EM’s Dr. Puneet Kapur (PGY5 EM, @Kapurp) was recognized for his stellar case submission involving identification and test performance of several transthoracic echo findings as they relate to identifying acute pulmonary embolism. Many of you have heard of the value of each of the following findings as they relate to distinguishing acute from chronic RV strain: 
Here are clips from the actual case that show RV dilation in the PSL and McConell’s sign in the A4C. Despite these – it may remain challenging to reliably determine acute vs chronic strain (see details in the cited article below).
Well, don’t give up hope – introducing RVOT systolic excursion! This measurement is obtained using the parasternal short axis view at the level of the aortic valve.
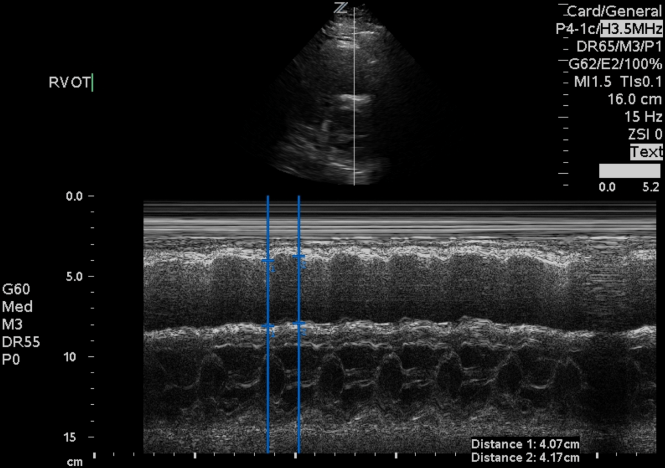 It appears that measuring RVOT systolic excursion (as a percentage of end-diastolic RVOT diameter minus end-systolic RVOT diameter divided by end-diastolic RVOT diameter) is both specific and highly sensitive for acute PE. Analysis of right ventricular outflow tract systolic excursion showed that a value <24.3% can be found in acute pulmonary embolism patients with 100% sensitivity and 95.56% specificity (AUC = 0.987, P < 0.0001).
It appears that measuring RVOT systolic excursion (as a percentage of end-diastolic RVOT diameter minus end-systolic RVOT diameter divided by end-diastolic RVOT diameter) is both specific and highly sensitive for acute PE. Analysis of right ventricular outflow tract systolic excursion showed that a value <24.3% can be found in acute pulmonary embolism patients with 100% sensitivity and 95.56% specificity (AUC = 0.987, P < 0.0001).
Sounds promising – looking forward to hearing and learning more about this.
We’re proud of Puneet! And while we’re at it – big thanks to the team at POCUS-Toronto for giving trainees like Dr. Kapur an opportunity to learn and excel in emergency POCUS.
Want to learn more about RVOT systolic excursion and acute RV strain? Check out the article below:
- Lõpez-Candales A, Edelman K. Right ventricular outflow tract systolic excursion: A distinguishing echocardiographic finding in acute pulmonary embolism. Echocardiography. 2013;30(6):649-657. doi:10.1111/echo.12120.
SASKSONO18 – RESUSONOLOGY
We’re live!
 REGISTER HERE
REGISTER HERE

You can also check out our trailer below!
You will be able to link to registration and find more details (including objectives and format) here: https://sasksonic.com/sasksono/
Upcoming Courses
We’ve got a great line up of courses to heat things up during the winter months!
Echo Guided Life Support (EGLS) – Saskatoon, SK. Dec 8th, 2017- registration is now open on the website. Register here
The EDE course (Plus) – North Battleford, SK, Jan 13th, 2018 – registration here
We will also be hosting another EGLS course on March 2nd in Saskatoon (as a pre conference workshop prior to SASKSONO18). Registration will open Dec 11, 2017.
Cheers,
The SASKSONIC Team
SASKONO18 – Welcome to Resusonology!

This year’s SASKSONO conference (SASKSONO18) is shaping up to be pretty exciting with a focus on resuscitative ultrasound (aka Resusonology). Whether you’re a rural doc covering the ED, in flight (HEMS/Air Ambulance), an emergency physician in an urban centre, or a hospital-based clinician managing patients in shock – this is the conference for you! Registration opens Dec 11, 2017!
CONFERENCE LEARNING OBJECTIVES
Participants will be able to:
- Describe the role of clinical ultrasonography in the care of acute and critically ill patients – specifically the application of focused transthoracic and transesophageal echocardiography in the management of patients in shock.
- Draw the right conclusions from new data – focusing on patient safety and improved diagnostic accuracy.
- Effectively communicate resuscitative ultrasound findings to colleagues ranging from pre-hospital to ED and beyond.
- Apply learning in hands-on and simulation sessions to mprove technique and interpretation of scans as well as exploring the choreographic implications associated with the clinical integration of ultrasound to resuscitation.
We kick the weekend off with Echo Guided Life Support (EGLS) as our pre-conference course on Friday March 2nd, 2018. We then go into a largely hands-on and small group learning environment for much of Saturday’s official programming.
Here’s an overview – starting at 9 am sharp!
Opening plenaries: Drs. Tom Jelic and Joann Kawchuk review the key indications, approaches and outcomes associated with resuscitative POCUS in a variety of environments.


Morning concurrent workshops include the FUNdamentals (ideal for students and novices – an 80 minute supervisedscanning session covering all shock related POCUS applications) and the Cutting Edge (designed for residents and clinicians, simulation- based small-group learning workshops delving into the clinical integration of TTE and TEE)

Afternoon concurrent sessions include more FUNDamentals (Lightning Abstracts and Sonogames) and a Resuscitative POCUS SKanapalouza (directly supervised scanning practice for participants who have attended a nationally recognized course- this session costs extra and space is limited)
Final plenary – putting it all together! Details are top secret for now – let’s just say were aiming for dramatic effect.
All done by 4:15 pm!
World Congress of Ultrasound in Med Ed – The Student Experience!

As a group of students, we had only learned about the World Congress of Ultrasound in Medical Education Conference (WCUME17) a couple of months ago. We were excited to enter the Ultrasound World Cup and gauge where our ultrasound skills compared to other students and schools worldwide. It was incredible to see how involved other students and schools are in undergrad ultrasound medical education across the world. In addition, it was eye opening to see the neat technology emerging into the medical education sphere including video games, learning modules, wireless and gel-less ultrasound probes and augmented reality ultrasound all with the aim of making the process of integrating ultrasound into medical education easier and appealing.
Aside from learning that Dr. Olszynski’s poutine record is three poutines in 24 hours, it really was an experience saturated with quality learning of multiple clinical ultrasonography applications including: Lung, MSK, Hemodynamics, Echo, and Family Medicine applications workshops that were attended by members of our two teams. These learning opportunities were invaluable because not only were we gaining new skills in the field of ultrasound, but we were learning these skills from some of the top doctors in ultrasound from across the world! It was great to be up close and personal with leaders in various fields and to receive their expertise regarding current and emerging ultrasound applications.
 Pictured above – the World Cup of Ultrasound Final with teams from Iran, USA and Canada (the Prairie Probes from USASK)
Pictured above – the World Cup of Ultrasound Final with teams from Iran, USA and Canada (the Prairie Probes from USASK)
The chance to compete against other students around the world in the World Cup of ultrasound was a blast – an experience full of challenges and key learning moments that we are sure will serve us well in our future medical careers. Both of the U of S teams did very well – which provided us with positive reinforcement with regards to the teaching we have receivedover the years in conjunction with our own self learning. We were thrilled to learn that one of our 2 teams (the Prairie Probes) had advanced to the World Cup of Ultrasound Final – representing both USASK and Canada on the world stage.
 Above – The teams, hosts and judges come together for a group photo
Above – The teams, hosts and judges come together for a group photo
It’s our hope that efforts to educate medical students in ultrasound continue to expand at the U of S with the ongoing support of the undergraduate ultrasound program. By speaking with other students we gained an even greater appreciation for the opportunities we have had to pursue and develop ultrasound skills. This conference provided another platform for us to increase our depth of ultrasound knowledge and meet some great people along the way.
Sincerely,
The Prairie Probes: Robert (Troy) Appleton, Anurag Dalai, and Andrew (AJ) Donauer
Scan Skatchewan: Eric Brenna, Rachit Batta, and Jeffrey Poon
PS: Soon after learning and being inspired by Dr. Olszynski’s poutine record, Team Scan-Skatchewan matched that feat as well!
SEMAC IX – SKanapalouza! Oct 14, 2017

SKanapalouza

A supervised scanning session that will cover all the core applications – expect to scan ~18 patients! Session starts at 1 pm and runs until 5 pm, Oct 14/2017– cost is $400.
email SASKSONIC@GMAIL.COM to reserve your spot!
Below is a map to the CLRC within the Health Sciences E Wing, Univ. of Saskatchewan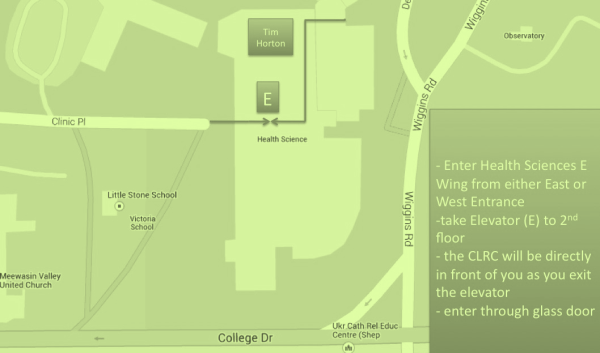
Welook forward to seeing you at the session!
THE SASKSONIC TEAM
SASKSONO18
This year’s theme will be resuscitative ultrasound – RESUSONOLOGY! And much like last year, we’ll be covering a range of applications from pre-hospital to ED to ICU. What more, not only will be offering lectures and workshops on focused transthoracic echo but we’ll also be discussing intra-operative transesophageal echo and we’ll be introducing intra-arrest TEE as well!
 Image modified courtesy of https://www.flickr.com/photos/29233640@N07/5088892415/
Image modified courtesy of https://www.flickr.com/photos/29233640@N07/5088892415/
Stay tuned – more details to come in the next few weeks!
Cheers,
Paul Olszynski
Keeping It Together!
Managing a portfolio/logbook of your training scans
As a former family physician/part time regional centre emergency room doctor, and as a physician who is currently refocusing on internal medicine and critical care (yes, I am back in residency), I am justifiably a point-of-care ultrasound (POCUS) enthusiast.
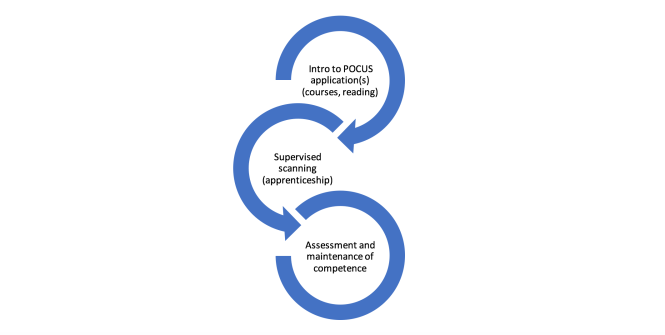
You are probably aware that various POCUS credentialing processes, specifically for those clinicians who did not receive longitudinal POCUS training during medical school or residency, often look somewhat like this:
Back in 2008, the University of Saskatchewan’s Department of Emergency Medicine embarked on a process much like the above by adopting the Canadian Point of Care Ultrasound Society’s (CPOCUS) certification program. It is currently the department’s primary POCUS credential, and it has served them well in terms of assuring basic competence amongst already-in-practice clinicians (over 80% of Emergency Physicians in Saskatoon have obtained basic CPOCUS certification). But as the number of acute care POCUS applications continues to grow – with now well established resuscitative, diagnostic and musculoskeletal applications – so too has the demand for robust training processes and improved training workflow. Incidentally, this same department just launched its own internal wireless image capture system (QPath) thus enabling a pretty slick training regime, but this post is for those eager POCUS learners whose departments aren’t quite there (yet).
One important evolution in these newer training schemes is the increasing role of image capture (specifically capture of real patient clips). CPOCUS, for example, now accepts up to 50% of training scans (of advanced applications) in the form of saved clips for review by their instructors.
To comply with the option of obtaining additional scans for review by your supervisor/ instructor, I do the following: I record de-identified clips, approximately 4 seconds long and insert them into presentation software. Choosing a convenient “split screen” slide, allows a video clip on the one side and an interpretation on the other. This is preceded by a short clinical vignette and rounded off with a short diagnostic summary.
I find that this keeps my clips and case information together and produces a visually pleasing, easy to follow log of my un-proctored scans. Reviewers can use the notes area for critiquing, questions or suggestions. Here is what a typical case ends up looking like:
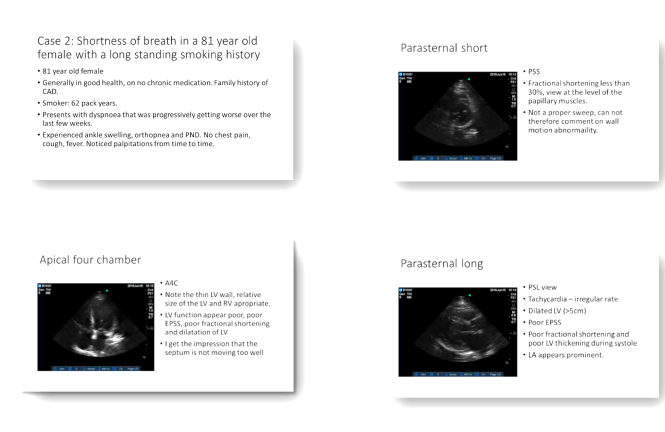
The few slides above illustrate a picture of an elderly lady with a longstanding smoking history presenting with shortness of breath. Her cardiac views would suggest a cardiac etiology as opposed to COPD for her symptoms. Scanning her lungs showed B lines in all fields. Her formal echocardiography was consistent with my bedside assessment and reported an EF of 30%. As a result of POCUS, heart failure treatment was initiated earlier.
This is how I keep my scans together. Feel free to use it! I would love to hear from others so please comment and tell us how you keep your scans together.
Dr Leon Byker, BSc MBChB CCFP; PGY2 Internal Medicine, University of Saskatchewan.
Peer Review by Dr. Paul Olszynski, Emergency Medicine, Director of Sasksonic, University of Saskatchewan
First fall POCUS course coming your way!
We’ll be hosting an EDE Course (Surgical – applications include scanning for pneumothorax, hemothorax, hemoperitoneum, pericardial effusion and abdominal aortic aneurysm) on Saturday, September 23rd at the CLRC of the Health Sciences Building.
Email sasksonic@gmail.com to secure your spot and arrange payment.
Cheers,
the Sasksonic team
