There has been A LOT of talk about POCUS governance lately – and at USASK we are right in there with a recent publication in The Ultrasound Journal on our efforts to develop a consensus-based multidisciplinary POCUS framework.
This Saturday @USASKEM and @usask_CME are hosting the 11th Saskatchewan Emergency Medicine Annual Conference (SEMAC XI) in Saskatoon, SK. We will be reviewing the recently adopted (province wide) Saskatchewan Emergency Ultrasound Guidelines: STANDARDS FOR EMERGENCY ULTRASOUND Final
These are in keeping (and in fact exceed) the above USASK POCUS Framework and are also well aligned with CAEP’s recent EM POCUS Position Statement.
Here’s the Executive Summary for the Sask EUS Guidelines:
Emergency ultrasound (EUS) comprises a set of focused applications utilized to diagnose life-threatening conditions, guide invasive procedures, and treat emergency medical conditions. [2] The proposed standards take into account that emergency care, and thus EUS, is within the scope of emergency physicians, family physicians and nurse practitioners. Given the significant contextual and resource differences between urban/tertiary centres and rural/regional sites, recommendations related to training, privileging and quality assurance are tailored accordingly.
These standards represent one of many initiatives developed to help ensure high quality training in, and use of, EUS in the province of Saskatchewan.

The USASK experience with logging scans and the EchoLog App
|

Big thanks to out-going USUS President Laura Neuburger for submitting this review!
Click on the link for a copy of the update: USUS 2018-2019 Update
We’re excited to be announcing the following fall courses:
The EDE course in Saskatoon, SK on Sept 22nd, 2019.
The EGLS Course in Saskatoon, SK has been scheduled for Oct 7th/2019.
To register or get more info, contact sasksonic@gmail.com
Stay tuned – details including dates and presenters will be coming soon!
REGISTRATION NOW OPEN: https://ccdeconference.usask.ca/index.aspx?cid=408
This year, our “DEEP DIVE” means we will be going beyond test performance metrics, exploring in-depth the role clinical ultrasonography can have in improving patient outcomes and system efficiencies. Our conference includes a range of learning experiences including short lectures, hands on workshops for beginners as well as those already familiar with the basics, a Sono-Round Table to develop a multidisciplinary clinical ultrasonography framework at USASK, supervised scanning with top level coaching, as well as rapid oral abstracts and the always entertaining Sonogames!
As organizers, we are committed to delivering a conference that supports the learning and wellness of all our attendees. We have included several optional opportunities for networking, exercise, relaxation and laughter! We will also have spaces for breastfeeding/pumping for those who may choose to use them, and as organizers, will do our best to help attendees secure quality childcare if needed. We also hope to be a low/minimal waste conference so please consider bringing your own coffee mug and/or water bottle.
7:30: Wellness Opportunity (optional) “Run at the speed of sound” or “Sound walk with talk”. We will provide a meeting location and encourage our attendee runners and walkers to join us for a great start to the day!
8:00 – 9:00 am: Registration and breakfast
9:00 am: Introductions and acknowledgement of our Treaty 6 commitment.
9: 15 am: Dan Kim – Deep Dive into EM POCUS
9:45 am: Dr. Peggy Lambos – Deep Dive into Pediatric POCUS
10:15 am: Nutrition break (Wellness oriented with healthy snacks offered)
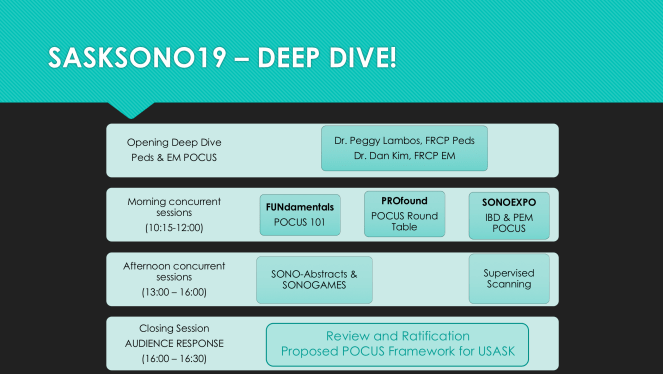
10:30 am – 12:00 pm: Morning Concurrent Sessions
FUNdamentals: POCUS 101 will be an introductory session for those new to clinical ultrasonography/Point of Care Ultrasound (POCUS). It will include flipped content sent to you before the conference as well as a quiz. The workshop will include a brief review ovf key concepts and hands on scanning practice of three core applications: scanning for abdominal and pleural fluid as well as pericardial effusion. Completion will include an assessment which, if passed, makes you eligible for more supervised scanning in the afternoon!
PROfound: USask’s first ever multidisciplinary POCUS Round Table will give Saskatchewan clinicians a chance to further guide the adoption and integration of POCUS throughout the province of Saskatchewan. We hope to establish provincial recommendations on training, scope of practice, documentation and quality assurance. Key recommendations will then be shared with the entire conference audience at the last session of the day for feedback and ratification. There will be flipped content sent out for this session including a draft framework document.
SONO EXPO: For those interested in exploring the spectrum of POCUS applications at USASK, we are excited to offer you deep dives into Inflammatory Bowel ultrasound as well as Pediatric EM ultrasound. And as usual, expect at least 30 minutes of hands on scanning and anatomy learning as well! This is a great opportunity for students and residents to explore applications outside the core USASK POCUS curriculum.
12:00 pm – 1:00 pm: Break which includes a nutritious lunch, an optional stretching session, opportunities to connect with old friends and/or make new ones!
1:00 – 4:00 pm: Afternoon Concurrent Sessions
SONO Abstracts and SONOlympiad: Always inspiring, educational and a good time, the students square off with their abstracts and then go head to head in the sonogames.
1:00 pm: SonoAbstracts
2:00 pm to 3:45 pm : SONOlympiad

SUPERVISED SCANNING: Struggling with an application or two? Need some POCUS coaching? Here’s your chance! Instructors qualified in basic, diagnostic and resuscitative POCUS will be on hand to help you take your scanning to the next level for 3 straight hours! And if that seems a bit daunting – don’t sweat it, we’ll offer a mid-point stretch and re-energizing session. This way you’ll be sure to finish strong as you head into the final hour which will include (for section 3 credits) a detailed assessment of your skills!
4 pm: Closing session
SONO ROUND UP: We will present the main recommendations for a USASK POCUS Framework as developed by the Round Table panels and participants. The audience will have the opportunity to provide feedback and vote using an audience response system.

REGISTRATION NOW OPEN: https://ccdeconference.usask.ca/index.aspx?cid=408
CHECK OUT THE TRAILER!
Download the poster (with an active registration link) for distribution to your colleagues!


Still thinking about that back to school list?
Since point of care ultrasound is part of the curriculum, shouldn’t we provide all of our students with a convenient and safe way to track their scans and progress? We certainly think so!
We’re working on a plan with @EchoLog so stay tuned, more details to come in a couple of weeks!
Cheers,
The Sasksonic team